
For those of you who don’t know, I’ve had a few surgeries on my left shoulder after multiple dislocations in my late teens and early twenties, until there came a point that after a pick-up touch football game along the shores of the Chateauguay River, my shoulder fell out of socket after my making an overhead catch and landing on my shoulder – where everyone on the sidelines heard a pop… and after a visit to the hospital, the Doc confirmed the arm wasn’t going to go back into the socket without some intervention.
The Doctors performed what was called a Putti Plat Operation. The Putti-Platt procedure is a historically significant non-anatomic procedure for shoulder instability with promising initial outcomes but disappointing long-term follow-up. Obviously, what they know today is not what they knew back in 1978. The procedure is based on the concept of tightening the anterior capsule and subscapularis with a subsequent accepted loss of external rotation in order to increase the stability of the shoulder. In this procedure, the flexible cord (tendon) of the subscapularis muscle is cut and then reattached to the head of the upper arm bone (humerus). This procedure makes the head of the upper arm bone tighter to the shoulder blade allowing better stability of the shoulder joint. It’s not a surgery that would be recommended today if I had the same injury.
The Doctors told me they used five metal staples to hold mine in place back in 1970 something – I can’t even recall the year now but for some reason, I am thinking 1978. So 45 years ago…
For those 45 years, I mostly ignored it or worked around it – I knew I had limitations and it mostly affected my swimming but generally, it worked as a shoulder should. But after I hit sixty, it started to hurt more and more and last year, I finally made a visit to Dr. Olivia Cheng in Collingwood. Her prognosis was eloquent. She said, and I quote; “That is one ugly shoulder”.
So we agreed to have an MRI done and then discus my options. After getting back the results, Dr. Cheng’s opinion hadn’t changed but she did mention something that I decided would be a better option for me and that was to begin a strength training program rather than undergo a shoulder replacement. Dr. Cheng basically said, “How bad is the pain?” and I said, “Well, I’ve had it for 45 years now and it seems to be improving with strength training and swimming”. and she said – “Forget the operation. I’ll do it if you want it, but you may have to do it again in ten years if you keep on exercising like you do because you’ll wear it out. Come back and see me when you are 75 and we’ll check it again”.
Here the MRI Results;
First, a bit of an explanation. The Rotator cuff is a group of four muscles: Supraspinatus, Infraspinatus, Teres Minor and the Subscapularis.
These muscles originate at at the shoulder blade and attach to the head of the humerus. These muscles work together to maintain the desired position of humeral head on the glenoid, the articular surface of the shoulder blade. If the rotator cuff is not functioning properly, a simple maneuver like lifting your arm over your head will result in increased stress on the structures associated with the shoulder complex.
The Findings of my MRI – What is wrong with my shoulder inside of me…
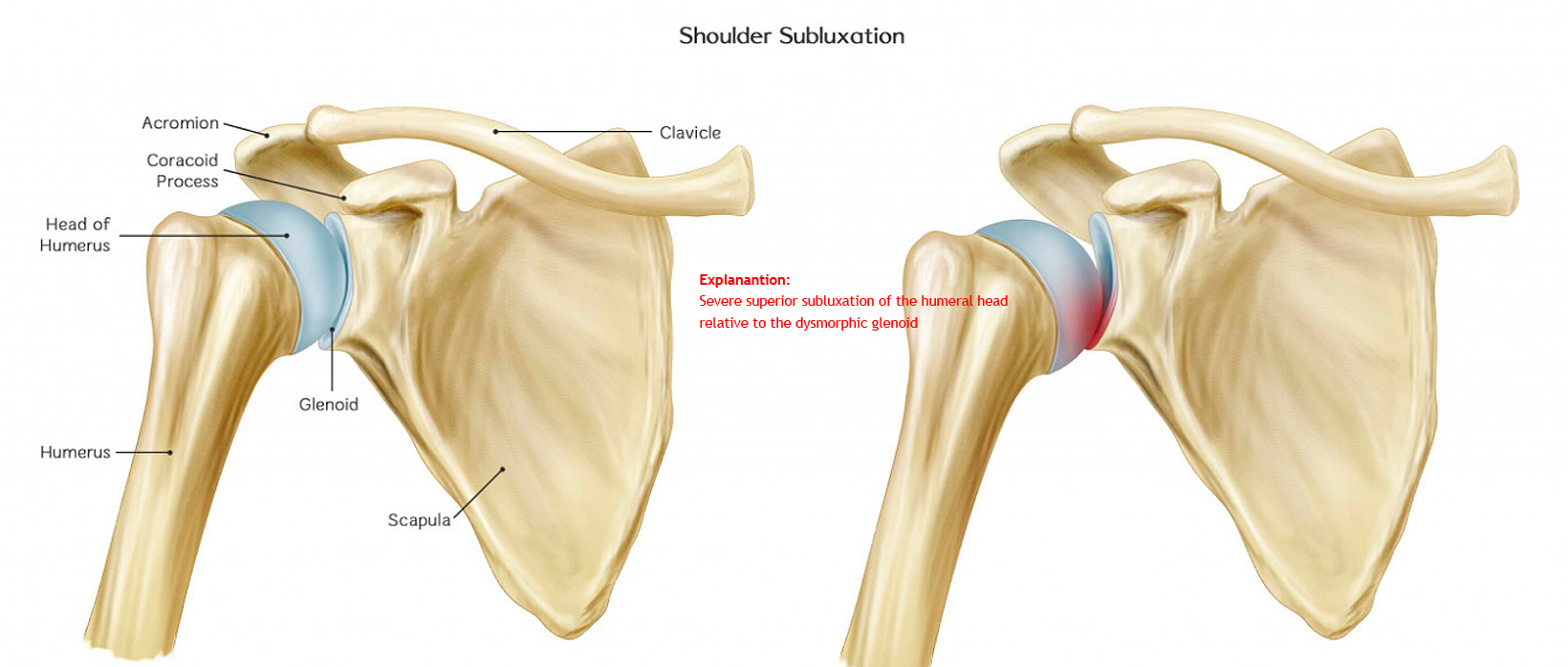
• There is at least moderate to severe grade left glenohumeral Osteoarthritis, with severe superior subluxation of the humeral head relative to the dysmorphic glenoid. There is severe restriction of the subacromial space. A subluxation is a partial dislocation within the body. This dislocation typically occurs in a joint, like my shoulder seen above. In other words, my humerus doesn’t really fit or stay in the Glenoid scoket very well. Plus, I have arthritis in there now.
• There is heterogeneity of the proximal left humerus and glenoid with features suspicious of advanced multifocal subchondral cystic change. A subchondral cyst is a fluid-filled space inside a joint that extends from one of the bones that forms the joint. This type of bone cyst is caused by osteoarthritis. It may require aspiration (drawing the fluid out), but the arthritis condition usually must also be addressed to prevent further cyst formation. I don’t think they are going to do anything about mine.
Osteoarthritis (OA) is the most common cystic change. It breaks down the cartilage. OA can happen from simple wear and tear over time, or because of a sudden injury to a joint, like mine after 45 years. Either way, the normal, smooth, gliding of one bone against another in your joints starts to cause more friction. That leads to the cyst.
Heterogeneity is not something to be afraid of, it just means that there is variability in the data. So, if one brings together different studies for analysing them or doing a meta-analysis, it is clear that there will be differences found. The opposite of heterogeneity is homogeneity meaning that all studies show the same effect. I hate having to figure out what the results mean by having to google search every single word.
• The remainder of the bone marrow signal intensities are within normal limits. This sounded like it was okay so I didn’t even bother to google it.
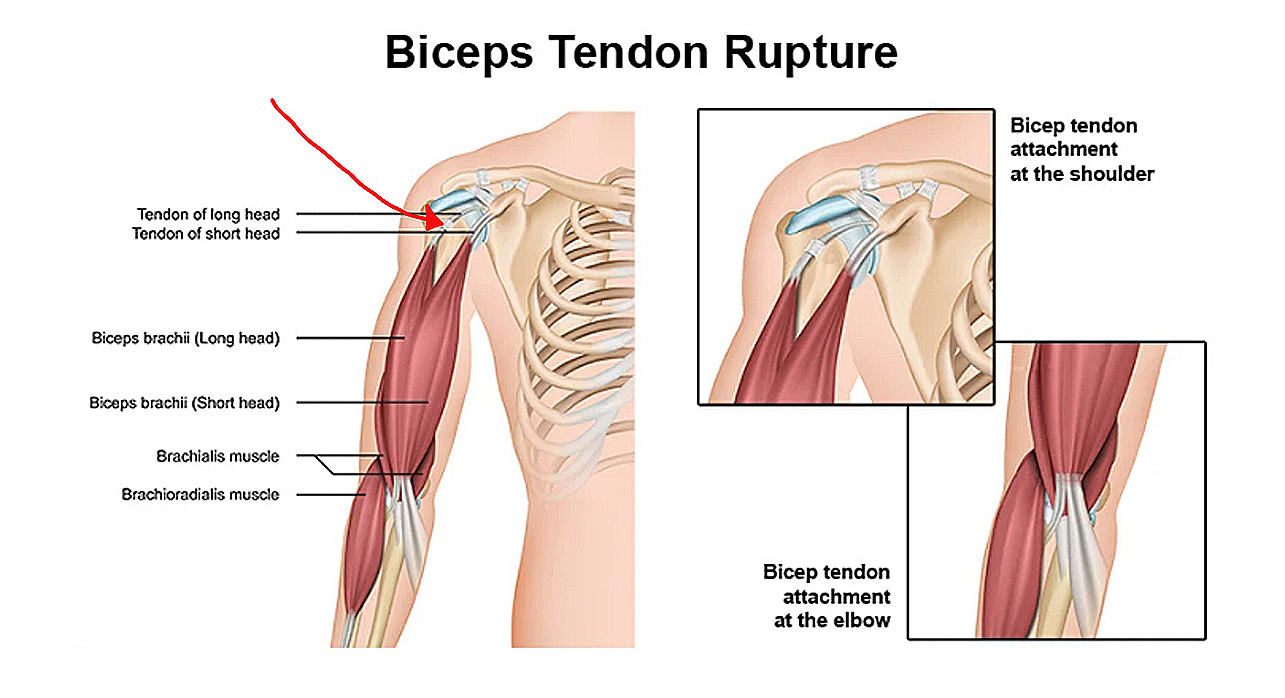
• There is either a Split Tendon (I’ve pointed this out with a red arrow on the sketch above) or a moderate length partial-thickness tear of the long head of the biceps tendon which is still within the inter-tubercular groove. There is significant degeneration of the biceps anchor and labra. Most research I’ve done seems to say that with proper exercise, I can maintain this or even build it back up. For those of you who are interested, your biceps tendons attach the biceps muscle to bones in the shoulder and elbow. If you tear the biceps tendon at the shoulder, you may lose some strength in your arm and have pain when you forcefully turn your arm from palm down to palm up.
The long head of the biceps tendon is more likely to be injured, which is my case. This is because it is vulnerable as it travels through the shoulder joint to its attachment point in the socket. Fortunately, the biceps has two attachments at the shoulder. The short head of the biceps rarely tears. Because of this second attachment, most people can still use their biceps even after a complete tear of the long head.
Basically, flexibility and strengthening exercises will restore movement and strengthen a shoulder with these issues so again, strength training and swimming is helping a great deal.
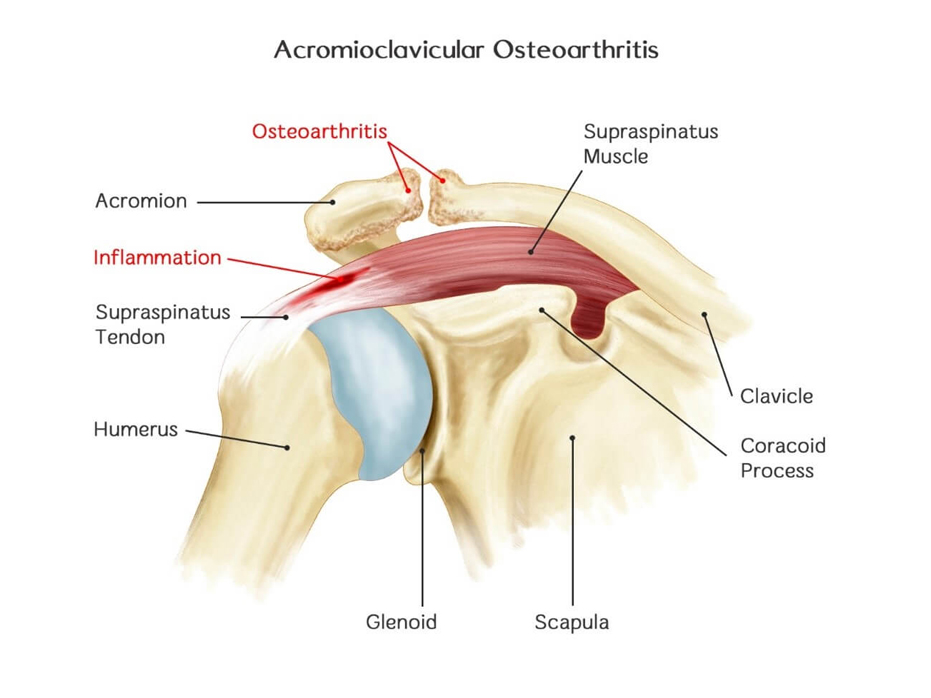
• The morphology of The Acromion is unremarkable however there is moderate Osteoarthritis of the right AC Joint. AC joint osteoarthritis of the acromio-clavicular joint is most common in people who are middle aged. It develops when the cartilage in the AC joint begins to wear out. With this condition, there is usually accompanying pain that limits the motion of the arm. My strength training and swimming seems to be maintaining the strength and allowing me to live fairly pain free at this point, although when I was working full time rather than exercising every day, the pain was quite severe.
• There is evidence of mild sub-deltoid bursal fluid.
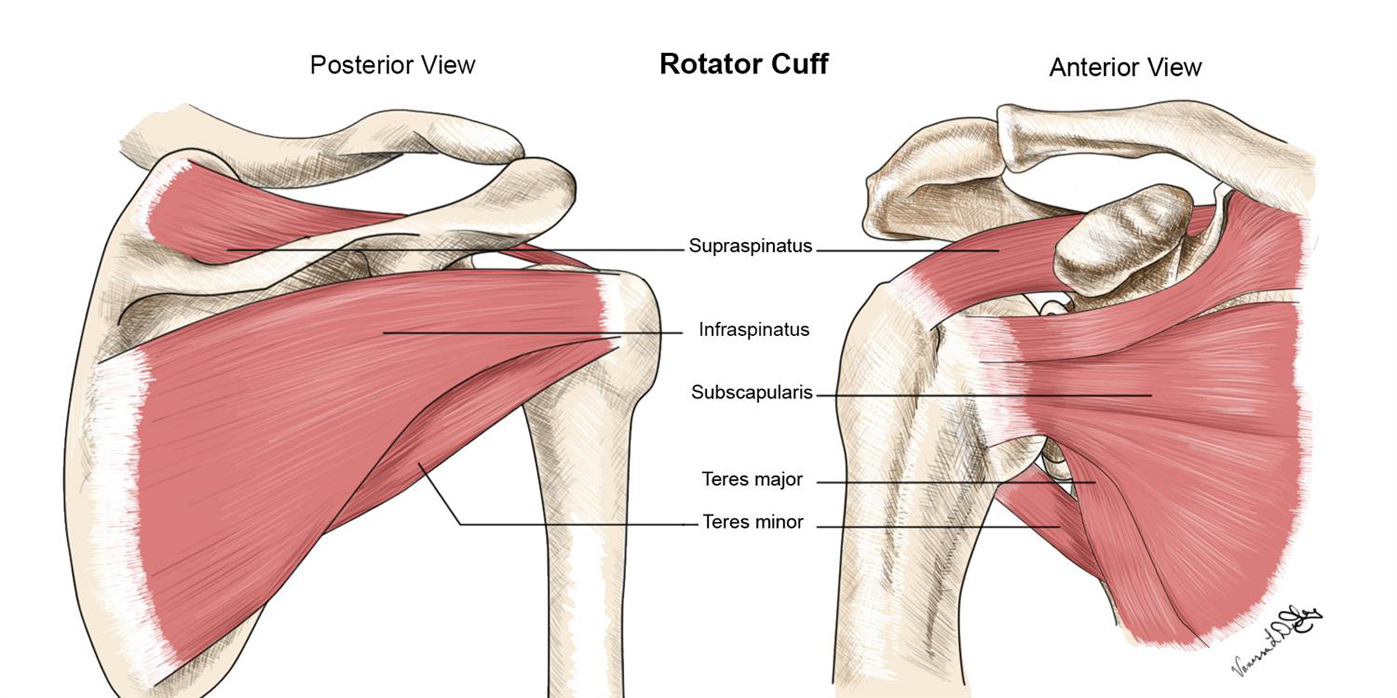
• The Left Subscapularis appears completely torn anteriorly and is terminal extent. To help explain that, I have added the sketch above. You can see at right what is called the anterior of the Subscapularis. Terminal extent means it is torn completely through. Dr. Cheng doesn’t think there is anything that can be done about this at this point in time.
• There is a high grade partial thickness tear involving the posterior half of The Supraspinatus and anterior third of The Infraspinatus. So based on the illustration above, that statement becomes fairly clear. You can see where those two tears would be inside my shoulder. The tear of the infraspinatus involves almost a third of the muscle. What I am working on in the gym is to strengthen what is left of these muscles in the hope that I still have some regenerative metabolism kicking around inside me with the right training.
In other words, I am hoping I can build the muscle back through diet and exercise.
—
Today, almost a full year after my results came back in, I am pleased to say that I am able to swim a full mile twice weekly without any shoulder pain. I am also able to strength train three times weekly with increasing weight across a fairly broad range of training exercises. Exercise and commitment have helped. My shoulders feel strong and I have little to no pain any longer.




No Comments